Esophageal Varices (Varicosities): Causes, Warning Signs & Treatment in Karachi
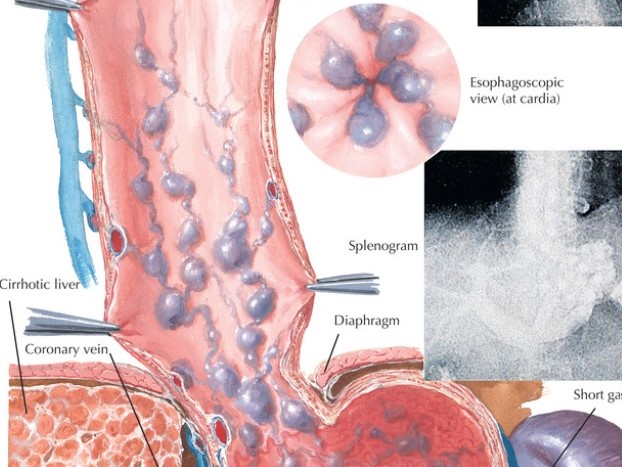
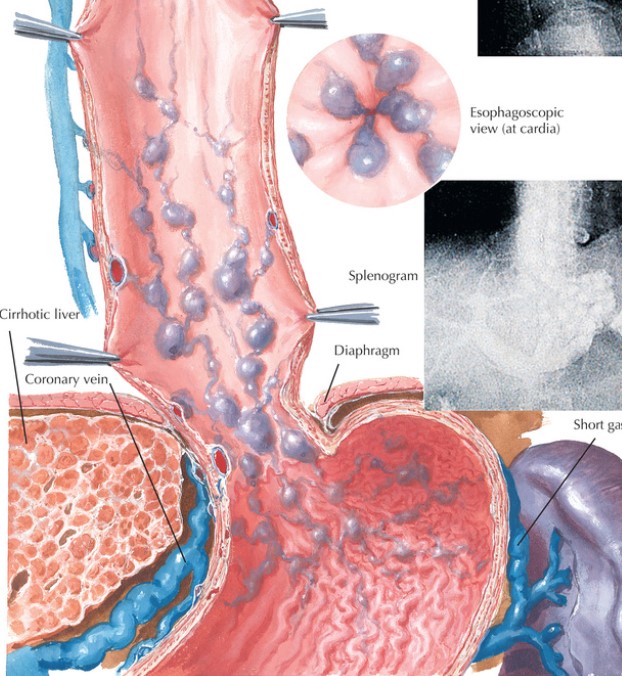
Esophageal varices — sometimes called esophageal varicosities — are swollen, fragile veins that form in the lining of the food pipe (esophagus). They develop when blood cannot flow freely through a damaged liver and is rerouted through smaller veins that are not designed to carry that volume. When these veins rupture, the result is sudden, severe bleeding that can be fatal without emergency treatment.
In Pakistan, where Hepatitis B and Hepatitis C are among the leading causes of liver cirrhosis, esophageal varices are a serious and underdiagnosed complication. Many patients have varices for years without knowing — until a bleed occurs.
Dr. Muhammad Ali Taj is a Consultant Gastroenterologist, Hepatologist, and Endoscopy Specialist with over 27 years of experience. He performs screening endoscopies and variceal treatments including Endoscopic Variceal Ligation (EVL/banding) at multiple hospitals in Karachi, including Ziauddin Hospital (Clifton) and Hill Park General Hospital.
Why Do Varices Form? Understanding Portal Hypertension
The key to understanding esophageal varices is portal hypertension — elevated pressure in the portal vein, which carries blood from the intestines to the liver.
In a healthy liver, blood flows through freely. In a cirrhotic (scarred) liver, this flow is blocked. Pressure builds up behind the blockage. The body attempts to bypass the damaged liver by routing blood through smaller veins — including those in the esophagus and stomach wall. These veins were never built for this volume of blood. They swell, weaken, and become varices.
The higher the portal pressure, the more advanced and dangerous the varices.
Causes of Esophageal Varices in Pakistan
In Pakistan, the most common underlying causes differ from Western populations:
1. Hepatitis C Virus (HCV) cirrhosis — Pakistan has one of the highest HCV prevalence rates globally. Decades of untreated Hepatitis C leads to cirrhosis in a significant proportion of patients.
2. Hepatitis B Virus (HBV) cirrhosis — Chronic Hepatitis B, especially when contracted at birth or in childhood and left untreated, is a major driver of liver cirrhosis and varices.
3. Non-Alcoholic Fatty Liver Disease (NAFLD) — Increasingly common due to obesity and type 2 diabetes, NAFLD can progress to cirrhosis over years without alcohol being a factor.
4. Autoimmune hepatitis and other causes — Less common but important to identify since they are treatable if caught early.
5. Alcohol-related liver disease — Less prevalent than in Western countries but present.
6. Schistosomiasis (bilharzias) — A parasitic infection affecting portal pressure, seen in some parts of Pakistan and rural areas.
Grading Varices: From Small to Life-Threatening
Not all varices carry the same risk. Gastroenterologists grade them to guide treatment decisions:
| Grade | Appearance | Bleeding Risk |
|---|---|---|
| Grade 1 (Small) | Slightly raised veins, collapse with pressure | Low — monitor with surveillance endoscopy |
| Grade 2 (Medium) | Tortuous veins occupying less than 1/3 of esophageal lumen | Moderate — prophylactic treatment often started |
| Grade 3 (Large) | Prominent veins occupying more than 1/3 of lumen | High — treatment strongly recommended |
The annual risk of a first variceal bleed is 5–15% for large varices. Once a bleed has occurred, the risk of re-bleeding within 6 weeks is over 60% without treatment.
Warning Signs Before a Bleed
This is what most patients search for — and it is genuinely difficult to know because varices themselves are usually silent. However, certain symptoms suggest that portal hypertension and varices may be present, and warrant urgent endoscopic evaluation:
- Vomiting blood (hematemesis) — bright red or coffee-ground coloured — this is a medical emergency
- Black, tarry stools (melena) — digested blood passing through the digestive system
- A history of liver disease, Hepatitis B or C, or cirrhosis with no screening endoscopy in the past 1–2 years
- Abdominal swelling (ascites) — fluid in the abdomen, indicating decompensated liver disease
- Jaundice — yellowing of the skin or eyes
- Easy bruising or prolonged bleeding from small cuts — the liver makes clotting factors, and a damaged liver cannot produce enough
- Enlarged spleen on ultrasound — the spleen enlarges in portal hypertension as it tries to handle backed-up blood flow
If you have any history of liver disease and have never had a screening endoscopy, you should have one. Most patients with large varices have no pain or warning — the bleed is the first symptom.
Diagnosis: How Varices Are Found
Upper Endoscopy (Gold Standard)
Endoscopy is the only reliable way to see varices. A thin, flexible camera is passed through the mouth into the esophagus, allowing direct visualisation and grading. The procedure takes 10–15 minutes and is performed under sedation.
Who should be screened?
- All patients with confirmed cirrhosis at the time of diagnosis
- Patients with Hepatitis B or C who have had the infection for more than 10 years
- Anyone with portal hypertension detected on imaging or clinical examination
Endoscopic Color Doppler Ultrasonography
Assesses blood flow in portal and esophageal vessels — useful for staging portal hypertension.
Fibroscan (Transient Elastography)
Measures liver stiffness as a non-invasive indicator of cirrhosis severity. Higher stiffness values correlate with higher portal pressure and greater variceal risk.
CT Portal Venography
Used in complex cases to map the portal venous system before surgical or radiological intervention (TIPS procedure).
Treatment Options: Prevention, Emergency, and Long-Term Management
Management of esophageal varices operates in three phases.
Phase 1 — Preventing the First Bleed (Primary Prophylaxis)
For patients with medium or large varices who have never bled:
Non-selective beta-blockers (propranolol, carvedilol, nadolol) — these medications reduce portal pressure by lowering cardiac output and causing splanchnic vasoconstriction. They are taken as daily tablets and have been shown to reduce bleeding risk significantly.
Endoscopic Variceal Ligation (EVL/Banding) — tiny rubber bands are placed around each varix through the endoscope, cutting off blood supply to the swollen vein. The vein withers and falls off within days. A full EVL course typically requires 2–4 sessions spaced 2–4 weeks apart. Dr. Taj performs EVL at Karachi hospitals.
Phase 2 — Emergency Management of Active Bleeding
A variceal bleed is a life-threatening emergency requiring hospital admission:
- IV vasoconstrictors (terlipressin or octreotide) — reduce blood flow to the varices within minutes of administration
- Emergency endoscopy — within 12 hours of admission, to achieve haemostasis with EVL or injection sclerotherapy
- Antibiotic prophylaxis — liver disease patients are at high risk of infection during GI bleeds; antibiotics reduce mortality
- Blood transfusion — cautious transfusion to maintain haemoglobin around 7–8 g/dL (over-transfusion worsens portal pressure)
- Sengstaken-Blakemore tube — a balloon tamponade device used as a bridge to endoscopy in catastrophic bleeds
Phase 3 — Preventing Re-Bleeding (Secondary Prophylaxis)
After a first bleed, the combination of beta-blockers + serial EVL is the standard of care. Sessions continue until all varices are eradicated.
For patients whose varices recur or who are at very high risk:
- TIPS (Transjugular Intrahepatic Portosystemic Shunt) — a radiological procedure that creates a channel inside the liver to decompress the portal system
- Liver transplant evaluation — for decompensated cirrhosis, transplant remains the definitive treatment
Treating the Underlying Cause
Varices are a complication of cirrhosis. Where the underlying cause is treatable, treating it reduces portal pressure over time:
- Hepatitis C: Modern Direct-Acting Antivirals (DAAs) achieve a cure rate above 95% in 8–12 weeks. Curing HCV in a patient with early cirrhosis can significantly reduce portal pressure and variceal risk.
- Hepatitis B: Antiviral therapy (tenofovir, entecavir) suppresses viral replication, slowing progression of cirrhosis.
- NAFLD: Weight loss, diabetes control, and dietary changes can reverse early cirrhosis in some patients.
Frequently Asked Questions
Can esophageal varices be cured? Varices can be eradicated with Endoscopic Variceal Ligation (banding), but they can recur if the underlying liver disease is not treated. Treating the cause — Hepatitis B, C, or NAFLD — alongside EVL gives the best long-term outcome.
If I have Hepatitis B or C, do I definitely have varices? Not necessarily. Varices develop only after significant liver scarring (cirrhosis). Many Hepatitis B/C patients never develop cirrhosis, particularly if treated early. But if you have had chronic Hepatitis B or C for many years, a screening endoscopy and fibroscan are strongly advised.
Is variceal banding (EVL) painful? The procedure is performed under sedation — you will be asleep and feel nothing. Mild throat discomfort or difficulty swallowing for 24–48 hours after the procedure is common, and is treated with simple pain relief.
How often do I need screening endoscopy after diagnosis? If no varices are found: repeat every 2–3 years (for compensated cirrhosis) or every year (for decompensated cirrhosis). If small varices are found: repeat every 1–2 years. If large varices are treated with EVL: repeat every 3–6 months until eradication, then every 6–12 months thereafter.
What is the survival rate for variceal bleeding? Six-week mortality for a first variceal bleed ranges from 15–25% in published studies. This number has improved significantly with modern treatment protocols. Patients who receive prompt endoscopy and pharmacological treatment within 12 hours have the best outcomes. Survival is also strongly influenced by the severity of underlying liver disease (Child-Pugh and MELD scores).
Can I take aspirin or ibuprofen if I have varices? No. NSAIDs (ibuprofen, diclofenac, aspirin for pain) significantly increase the risk of GI bleeding in patients with cirrhosis and portal hypertension. Paracetamol (acetaminophen) in standard doses is safer for pain relief. Always discuss any medications — including over-the-counter drugs — with Dr. Taj before taking them.
To book a screening endoscopy or discuss your liver health with Dr. Taj, contact us on WhatsApp 0312-3803935 or visit our contact page.